
Drug Withdrawal Timeline Simulator
How Long Will It Take?
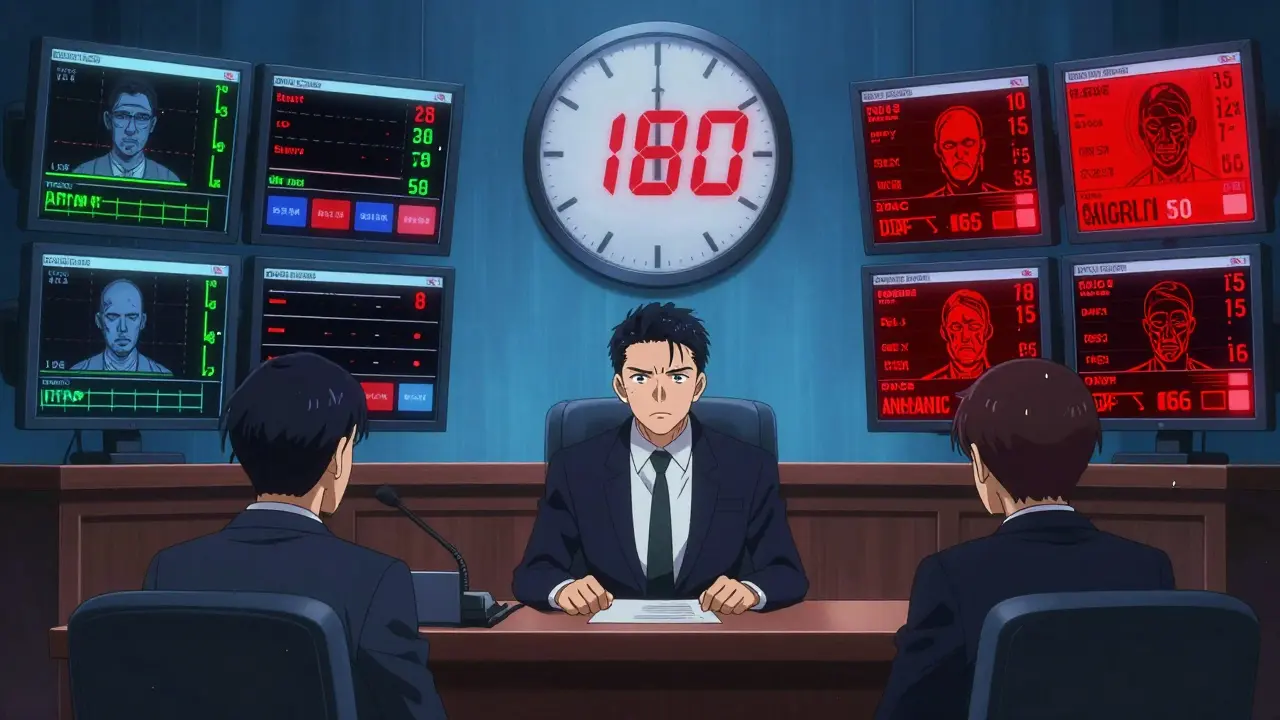
Compare the timeline for drug withdrawal before and after the 2023 FDA reforms. See how long it took for drugs to be pulled from the market under the old system versus the new rules.
Before 2023
Average: 46 months
After 2023
Average: 180 days
What does this mean?
The old system could take up to 4 years for a drug to be withdrawn after evidence of ineffectiveness. Now, the FDA must act within 180 days of evidence.
This change means patients are protected faster from drugs that don't work or cause harm.
Makena (Preterm Birth Drug)
Approved in 2011 based on small study showing slight reduction in early labor.
Withdrawal Timeline: 13 years after evidence showed it was ineffective.
ALS Treatment (2023)
First drug withdrawn under new law after confirmatory trials showed no benefit.
Withdrawal Timeline: Less than 6 months from evidence to removal.
Why this matters
Before 2023, about 41% of small cell lung cancer patients were treated with drugs that were later proven ineffective. Now, the FDA must act within 180 days.
If you're taking a new drug, ask your doctor:
- Was this approved under accelerated approval?
- Has the confirmatory trial been completed?
- Is there a public record of the trial results?
Every year, dozens of medications disappear from pharmacy shelves-not because they’re outdated, but because they’re dangerous. Or worse, because they never worked at all. The public rarely hears about these withdrawals until someone they know gets hurt. But behind every recall is a complex, often slow-moving system designed to protect patients. And for years, that system failed too many people.
How a Drug Gets Approved-And Why It Might Be Removed
The FDA doesn’t approve drugs because they’re safe. It approves them because the benefits outweigh the risks. That’s the rule. But for some drugs, especially those approved under the accelerated approval pathway, that balance is based on hope, not proof. These drugs are fast-tracked for serious conditions like cancer or rare diseases, where waiting for full clinical data could mean death. So the FDA lets them go to market based on early signals-like tumor shrinkage or a lab marker-that suggest they might help. But here’s the problem: those early signals don’t always mean real benefit. In fact, a 2022 study in JAMA Internal Medicine found that nearly 13% of drugs approved under this pathway were later withdrawn because they didn’t actually improve survival or quality of life. That’s not a glitch. It’s a design flaw. Take Makena, a drug approved in 2011 to prevent preterm birth. It was based on a small study showing a slight drop in early labor. But years later, a large, rigorous trial showed it did nothing. Still, the FDA waited over a decade to pull it. By then, around 150,000 women had been prescribed it. That’s not just a delay-it’s a failure.The Old System: Years of Waiting, Patients Left in the Dark
Before 2023, the FDA had no real timeline for withdrawing drugs. Once a sponsor failed to prove a drug worked, the agency could sit on the evidence for years. The average time to withdraw a drug after evidence of ineffectiveness was 46 months-almost four years. Meanwhile, patients kept getting prescriptions. Oncology drugs were the worst offenders. One study from Penn LDI found that 26% of all accelerated approval cancer drugs were eventually pulled. In small cell lung cancer, 41% of patients treated with these drugs got them even after they were proven useless. Doctors didn’t know they were prescribing a dead end. Pharmacies didn’t know to stop filling them. And patients? They had no idea. The system was opaque. The FDA didn’t always communicate clearly. A drug could be “withdrawn from sale” because the manufacturer stopped shipping it-but not because the FDA ordered it. Or it could be pulled for safety reasons, but only after dozens of adverse events piled up. There was no urgency. No accountability. Just paperwork.The 2023 Change: A New Law, Faster Action
Everything changed with the Consolidated Appropriations Act of 2023. For the first time, the FDA got real power to move quickly. Now, if a drug approved under accelerated approval fails its confirmatory trial-or if the company doesn’t even try to complete it-the agency can act in months, not years. The law sets clear triggers:- The sponsor fails to conduct required post-approval studies
- The studies don’t verify the drug’s benefit
- Independent data proves it’s unsafe or ineffective
- The company spreads false claims about the drug
Who’s Affected When a Drug Is Pulled?
It’s not just patients. Everyone in the system feels the ripple. Doctors have to switch treatments on the fly. One oncology practice reported it took an average of 72 hours just to find alternatives for patients on a withdrawn drug. Pharmacists scramble to update systems. Insurance companies deny claims for drugs that are no longer approved. And patients? They’re left wondering: Was I used as a test subject? One metastatic breast cancer patient wrote on a patient forum in 2022: “I was on [withdrawn drug] for 18 months. My oncologist said it was standard. Now we know it didn’t help.” That’s not rare. A 2023 Reddit thread on r/oncology had 142 comments. 87% of respondents said they worried they’d been prescribed a drug later pulled for being ineffective. The fear isn’t irrational. It’s based on history.Why Some Drugs Get Withdrawn-and Others Don’t
Not all withdrawals are the same. About 60% are due to safety issues-unforeseen side effects, organ damage, or death. The rest? Mostly because they don’t work. A small number are pulled for marketing fraud or manufacturing problems. But here’s the kicker: drugs approved traditionally-those with full clinical data before approval-are rarely pulled. The accelerated approval pathway is the problem zone. That’s where the risk is highest, and where oversight was weakest. The FDA’s own data shows that 40% of all accelerated approvals go to oncology drugs. That’s 80 drugs as of 2023. And of those, about 1 in 4 ended up being pulled. That’s a huge number of patients exposed to treatments with no proven benefit.
What’s Still Broken
The 2023 law is a major step forward. But it’s not perfect. First, it only applies to drugs approved after the law passed. That means Makena, and dozens of others approved before 2023, are stuck in the old system. The FDA still hasn’t acted on many of them. Second, the agency still doesn’t always communicate clearly. A 2023 FDA audit found only 42% of withdrawal notices included clear timelines for doctors and patients. That leaves too much room for confusion. Third, the FDA still relies heavily on sponsor-submitted data. Even with the new rules, it’s the drugmakers who run the confirmatory trials. And they have a financial incentive to delay bad news. Real progress will come when the FDA starts using real-world data-like prescriptions filled, hospital admissions, or patient outcomes tracked through electronic records-to monitor drugs after approval. A pilot program launched in January 2024 using data from Flatiron Health is a start. But it’s still small.What You Need to Know If You’re Taking a New Drug
If you’re prescribed a new drug for cancer, a rare disease, or another serious condition, ask these questions:- Was this approved under accelerated approval?
- Has the confirmatory trial been completed?
- Is there a public record of the trial results?
The Bigger Picture: Safety, Not Speed
The pharmaceutical industry argues that fast approvals save lives. And sometimes, they do. But we can’t trade safety for speed. The real innovation isn’t in getting drugs to market faster-it’s in knowing which ones actually work. The 2023 reforms are the strongest signal yet that the FDA is starting to take this seriously. But the test isn’t in the law. It’s in the action. Will the agency move quickly when the next Makena comes along? Will it stop waiting for paperwork and start acting on data? Will it protect patients before they’re harmed-or only after? The answer will tell us whether this change was just a policy update-or a true turning point.What’s the difference between a drug recall and a drug withdrawal?
A drug recall happens when a specific batch or lot of a drug is pulled because of contamination, labeling errors, or manufacturing issues. It’s usually limited and temporary. A drug withdrawal is when the FDA removes the entire drug from the market because it’s unsafe or ineffective. This isn’t about a bad batch-it’s about the drug itself. Withdrawals are permanent unless the company reapplies and proves safety and effectiveness.
Can a drug be pulled even if it’s still being sold?
Yes. The FDA can order a withdrawal even if the manufacturer hasn’t stopped selling it. In fact, the agency often has to force companies to stop distribution. Once the withdrawal is official, pharmacies can’t legally dispense the drug. Any remaining stock must be returned or destroyed. Patients who still have it should stop using it immediately and contact their doctor.
How do I know if a drug I’m taking was withdrawn?
Check the FDA’s Orange Book online. It lists drugs and their approval status. If a drug is marked as “withdrawn from sale for reasons of safety or effectiveness,” it’s no longer approved. You can also ask your pharmacist or call the FDA’s Drug Information line. Many hospitals and clinics now flag withdrawn drugs in their electronic prescribing systems, but not all do. If you’re unsure, don’t guess-ask.
Why do some drugs stay on the market for years after they’re proven ineffective?
Before 2023, the FDA had no legal deadline to act. It could take years to gather evidence, review it, notify the company, and go through appeals. The process was slow, bureaucratic, and often ignored by the public. Even after a trial showed a drug didn’t work, the agency might wait for more data-giving companies time to argue, delay, or push alternative interpretations. The result? Patients kept getting prescriptions that offered no benefit, only risk.
Are generic versions of withdrawn drugs still available?
No. Once a brand-name drug is withdrawn for safety or effectiveness reasons, generic versions can’t be approved or sold as substitutes. The FDA removes the drug from the Orange Book as a reference product. This means no generics can legally enter the market. If you see a generic version of a withdrawn drug, it’s either counterfeit or illegally distributed.



















Comments (16)